



Worldwide, patient engagement is becoming a “must do” for academics, industries and policy makers in the healthcare arena. The academic and managerial “buzz” on patient engagement is growing at a dizzying pace. In 2015, 665,300 new web indices were found on Google.com with the key words “patient engagement,” including 1,230 news pages and 6,200 dedicated blogs. During this same period, over 3,500 new academic papers focused on patient engagement.
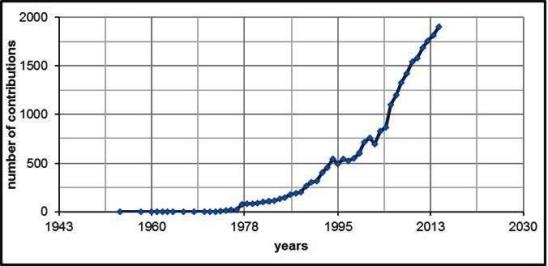
Trend of Google Scholar Sources indexed with Patient Engagement, 1954-2014
In Search of a Definition
The idea of patient engagement is based on the assumption that making patients/clients co-producers of their health can enhance their satisfaction with the healthcare system, as well as their responsibility in care, cure and prevention. However, despite this growing interest, a shared definition of patient engagement has yet to come and, as a consequence, concrete guidelines for practices are still awaited.
The question spontaneously arises: Is patient engagement a fashionable claim or a real guidance for practice?
Absence of the Patient Perspective
It’s curious to note that in this attempt to define patient engagement and how it can be achieved, patients are often absent, and scarce attention has been paid to their perspectives. Evidence-based studies aimed at giving voice to patients, their experience and their willingness to engage in their care and cure have been largely neglected so far. From our perspective, this lack of theoretical foundation represents a lost opportunity for really innovating and improving healthcare services sustainability.
The Critical Questions
How can we see engagement through patients’ eyes? How can we gain insights for orienting healthcare actions and addressing policies priorities?
It’s a Matter of Psychology
The discipline of consumer psychology is defined as the study of processes that individuals, groups or organizations enact to select, secure, use and dispose of products, services, experiences, or ideas to satisfy their needs and to fulfill their goals and values. This field can offer interesting cues to move forward in the modeling the subjective experiences of patient engagement. Deeply unveiling the patients’ processes of decision-making about their health-related conduct, desires and unmet needs regarding care services and well-being support, may cast light on some interesting conditions that hinder or support patient health engagement.
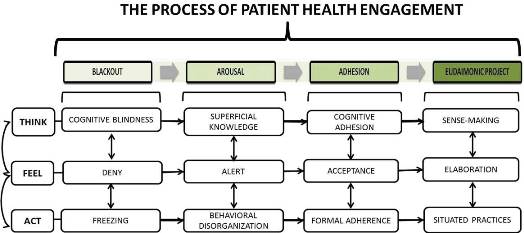
The Patient Health Engagement Model
By adopting a consumer psychology perspective and drawing on more than 10 years of research and practice dedicated to the in-depth understanding of patients’ perspectives about their illness journeys, we developed a conceptual model, called the Patient Health Engagement Model ( PHE model).The PHE model may be particularly useful to understanding patient/consumer engagement and how it develops.
Specifically, we define patient health engagement as a multi-dimensional psychosocial process resulting from the conjoint cognitive, emotional, and behavioral enactment of individuals toward their health conditions and their management. (Graffigna et al., 2014; Graffigna, Barello &Triberti, 2015).
Patient health engagement is a dynamic and evolutionary process that helps patients to resume a more active role in their lives and enjoy a better quality of life—even with their condition. The patient engagement process features four experiential positions. This evolutionary view of the patient engagement process suggests that a fully engaged patient results from a series of emotional (feel), cognitive (think), and behavioural (act) reframing of his/her health condition, and the success of the patient in advancing along this process depends on how he/she succeeded in previous phases.
In particular the process of patient engagement develops in four sequential phases of understanding and emotional adjustment to the disease or condition: blackout, arousal, adhesion, and eudaimonic project.
The Patient Health Engagement (PHE) Model, Adapted from Graffigna, Barello & Triberti, 2015
- Blackout: This is a pre-phase of disengagement at the onset of the disease when patients feel blocked and at the mercy of the healthcare system. They tend to deny the diagnosis and appear unable of making sense of their health condition. They are emotionally “frozen” and are not equipped to take over care and cure management. In this phase, it is crucial to help patients become aware of the problem and provide an initial educational toolbox to mobilize them to care for themselves.
- Arousal: In this phase, we see patients start to arouse, perceiving themselves as “ill bodies” but still delegating the majority of power to the healthcare system. At an emotional level, patients feel alerted and scared about their status, but they still haven’t enough cognitive elements to make of their health condition. As a result, they behave in a disorganized manner and are unable to manage their own health prescriptions. In order to sustain the evolution to the next phase, it is crucial to support patients emotionally by offering tailored psychological support to patients and their caregivers and helping them in understanding and accepting the diagnosis.
- Adhesion: A phase of formal “adhesion” or adherence to medical prescription follows. Here, patients have finally accepted the diagnosis and learned sufficient knowledge about the disease and its treatment to make them adequately skilled. However, they still appear unable to fully make sense to prescriptions and to manage them on their own. Patients, thus, are formally accepting of the treatment but not “on board” in the management of their own care. In order to move forward in the process, patients need help to more fully understand and metabolize the rationale behind prescriptions, participate in the decision-making process, and they need to be supported with tailored devices for self-management and prevention practices.
- Eudaimonic project: This is the final phase where patients are fully engaged and become co-designers of their health. They become able to perceive themselves as whole persons, positively included in their social context and able to follow meaningful practices of health management despite their diagnosis. In this phase, patients have come to fully understand their condition and feel sense of control over its course and treatment. In order to sustain this position, individuals need continuous counseling and targeted information to empower their sense of agency and become effective in “engaging” their healthcare system in positive co-planning of their health and well-being.
Opportunities to Innovate Healthcare
The PHE model, thus, enables us to easily capture the main features of the patient engagement experience. The evolution from one phase to the next may vary in time, depending on the individual patient and the context in which he or she is embedded. Furthermore, this process is not always linear. Patients may become stuck for longer periods in one phase or even retrocede to a previous phase if faced with additional traumatic events.
A Compass for Healthcare Professionals
The PHE model, however, offers an important support for healthcare professionals and managers to comprehend the stage where their patients are and help them plan effective and sustainable patient-centered interventions that truly improve patient autonomy and competence in managing their health. Specifically, the PHE model was conceived as a compass to orient the assessment of patient engagement in clinical consultations, to unveil patients’ healthcare service expectations and unmet needs to plan new services and to assess the engagement goals achieved by specific interventions.
Let’s see how this works in detail.
The PHE-Scale: Measuring Patient Engagement
Based on the model, we developed the PHE-Scale (Graffigna et al., 2015) allows a clinician to briefly and easily assess the patient’s clinical position by asking four straight-forward questions to gauge their psychological attitudes toward his/her health condition. This set of questions and the corresponding answers guide clinicians, managers and other professionals in dealing with interventions aimed at sustaining patients’ self-care abilities by assessing their primary psychological needs and care expectations.
Basically, the PHE-Scale questions the patients’ stage of psychological understanding of their compromised health condition and of their engagement needs (how they“feel”) when reflecting on their health status). This scale is the only specifically dedicated tool available today for assessing the degree of emotional understanding and adjustment reached by the patient concerning his/her own health condition when engaging in health management.
The specificity of this scale allows the clinician to not only to assess the actual patient’s attitude towards his/her health condition, but also to forecast the patient’s risk for disengagement in health management. Thus, the clinician can design a preventive targeted intervention to optimize care pathways.
A New Style of Interaction
This tool allows clinicians to move from a style of interaction that is clinician-directed and focuses on patients’ adherence to treatments, to one that supports patients’ motivation and autonomy in the care process, matches patients’ level of engagement, and ultimately increases engagement.
Editor’s Note: For a deeper understanding of how the PHE model is applied, watch for a follow-up contribution from Dr. Graffigna in April. In the meantime, you can learn more by visiting her website at http://docenti.unicatt.it/ita/guendalina_graffigna/ or consider these additional readings:
- Graffigna, G., Barello, S., Bonanomi, A., Menichetti J. (2016) The Motivating Function of Healthcare Professional in eHealth and mHealth Interventions for Type 2 Diabetes Patients and the Mediating Role of Patient Engagement. Journal of Diabetes Research http://www.hindawi.com/journals/jdr/2016/2974521/
- Graffigna, G., Barello, S., Triberti, S. (2015). Patient Engagement: a consumer centered approach. Degruyter Open http://www.degruyter.com/viewbooktoc/product/466090
- Graffigna, G., Barello, S., Bonanomi, A., Lozza, E. (2015) Measuring Patient Engagement: Development and Psychometric Properties of the Patient Health Engagement (PHE) Scale. Frontiers in Psychology. 6:274 http://journal.frontiersin.org/article/10.3389/fpsyg.2015.00274/abstract
- Barello S., Graffigna G. (2015) Engaging patients to recover life projectuality: An Italian cross-disease framework. Quality of Life Research http://link.springer.com/article/10.1007%2Fs11136-014-0846-x
- Barello S., Graffigna G. (2015) Patient engagement in healthcare: pathways for shared decision-making. Neuropsychological Trends http://www.ledonline.it/NeuropsychologicalTrends/allegati/NeuropsychologicalTrends_17_Barello.pdf




1 Comment
Thanks so much for sharing your expertise and research in this area. Shared decision making is critical to the future of health care!