




Virginia Mason is an urban integrated health system in the Puget Sound, Washington region, with our flagship campus located in downtown Seattle. Like most healthcare organizations, we strive to actively engage patients in their clinical care.
 We are guided by our strategic plan that puts the patient at the top of its pyramid format to influence all that we do and by our lean management method, the Virginia Mason Production System (VMPS). A key tenet of our lean-inspired management system is that the customer defines value.
We are guided by our strategic plan that puts the patient at the top of its pyramid format to influence all that we do and by our lean management method, the Virginia Mason Production System (VMPS). A key tenet of our lean-inspired management system is that the customer defines value.
With our long-term commitment to these foundational elements, we began rethinking how we could truly engage deeply with our customers as we seek to improve their experience of care.
A Three-Pronged Approach
Our work over the past few years has centered on the following strategies to directly involve patients and families in helping improve services and processes:
(1) Growing use of ethnographic experience-based design (EBD) methods to understand the emotional experiences and touch points of patients and families.
Dozens of EBD studies have been conducted and used to inform improvement projects. Most are small-scale, although we’re able to leverage EBD-trained leaders for larger-scale and organizational initiatives.
(2) Establishing a patient-family partner program that systematically embeds these volunteers in improvement work to co-design solutions together.
 We currently have 156 on-boarded volunteers ready to contribute to improvement activities. They sign up for opportunities through an electronic “job board.” We also push out notifications. Activities include participating on workshops, serving as members on committees and guiding teams, reviewing educational materials, speaking and presenting, and helping design curriculum. Most surprising and equally exciting is what we’re experiencing with access to these skills-based patient-family volunteers. While they initially sign up due to particular care experiences, many then contribute their broader knowledge and skills. We have patient-family partners with backgrounds, for example, in engineering, finance, business, healthcare, technology start-ups, legal, instructional design, construction and academia. Patients and families also are coming up with new ways they want to be involved, such as designing and teaching a class about how to deliver bad news to patients and enrolling in our VMPS training.
We currently have 156 on-boarded volunteers ready to contribute to improvement activities. They sign up for opportunities through an electronic “job board.” We also push out notifications. Activities include participating on workshops, serving as members on committees and guiding teams, reviewing educational materials, speaking and presenting, and helping design curriculum. Most surprising and equally exciting is what we’re experiencing with access to these skills-based patient-family volunteers. While they initially sign up due to particular care experiences, many then contribute their broader knowledge and skills. We have patient-family partners with backgrounds, for example, in engineering, finance, business, healthcare, technology start-ups, legal, instructional design, construction and academia. Patients and families also are coming up with new ways they want to be involved, such as designing and teaching a class about how to deliver bad news to patients and enrolling in our VMPS training.
(3) Integration of these strategies into our VMPS improvement methodology. We strive to combine the emotional experiences and stories from our customers with analytical improvement data such as lead times, wait times, cycle times and such. Negative emotional experiences are conveyed as a “defect” in our processes needing attention. Positive and negative experiences, along with patient-family needs and preferences, are included in visual depictions such as value stream maps and process flows.
Case Example: ALS Care
Here’s an example of how these strategies can unfold. The team at Bailey-Boushay House provides care for HIV, AIDS and other terminal diseases, including Amyotrophic Lateral Sclerosis (ALS or Lou Gehrig’s disease). They wanted to innovate around the care of ALS patients suffering from Frontotemporal Dementia (FTD) as a symptom of their disease. While the literature described FTD as a real diagnosis, no one had yet identified care strategies to support the patient and family. The team wanted to develop its expertise for this need. Goals included minimizing patient emotional outbursts, increasing patient independence and reducing staff anxiety.
Illuminating Critical Touch Points
The team started by involving family members of patients who had passed away, gathering the stories of their experiences. This illuminated critical touch points and emotional impacts being experienced by patients and their loved ones. Touch points are the experiences that leave lasting positive or negative memories because they represent what really matters to someone.
Using these insights and data gathered from staff, the team created what we call an experience questionnaire. This was used to gather more specific input from the clinical team.
All of the experience-based design data were integrated with information gathered from expert interviews and a literature search, along with data such as patient safety incidents, patient complaints, staff evaluations, process flows and cycle times. Details were shared with facility staff during a series of retreat sessions.
Developing Interventions
Next came a workshop and series of rapid tests of change involving patients and families to develop interventions that build trust between patients and caregivers, personalize care, and increase feelings of physical and psychological safety. Examples include:
- Family rooms for care companions to decompress and rest.
- Staff helping a patient and their family do a “monthly outing” of their choosing. These are mini “make a wish” type outings of normalcy. Examples have included taking a van with support equipment and staff to a planned route to view holiday lights around town (hot chocolate included), a baseball game, museums and even a night at the theater with dinner.
- Initiatives to help staff reframe, reset and get support when encountering challenging patient behaviors such as being “fired” from delivering that person’s care.
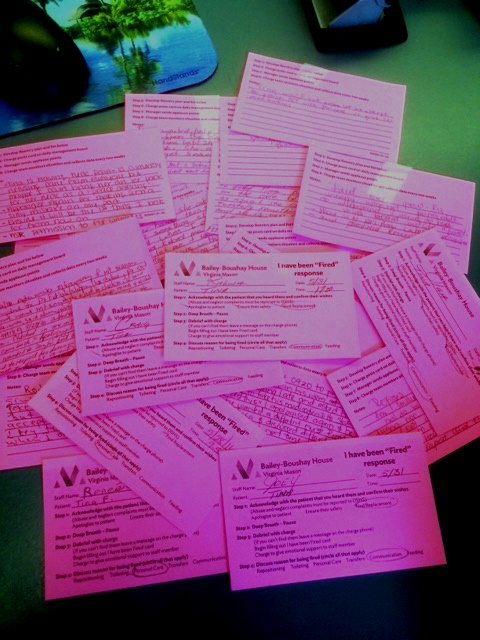
“I’ve been fired” cards that staff complete when a patient frustrated with their declining health situation takes out the anger on a caregiver. This triggers help from the charge team so the patient is still getting needed care and the staff member feels supported in a difficult situation.
Some Lessons to Share
The learning is constant when it comes to involving patients and families in improvement efforts. Some of it is procedural, and some of it is cultural. A few items to pass along:
- Expect patients and families to challenge deeply held assumptions you don’t even know you have. This is the big gift that comes with involvement. Really be open to their questions, observations and ideas—this is why you’ve invited them to the table, after all.
- Treat patients and families as equal members of improvement teams. They are driven by a desire to give back and help other patients and families have better care experiences. They don’t want to be treated with kid gloves.
- Expect some leaders to say “no thanks” to the offer of having patients and families help with their improvement work. They’re not trying to be disrespectful. They just really don’t think that level of involvement is needed on certain projects, especially behind-the-scenes processes. Take a long-term view in helping more leaders get comfortable with saying yes.
- Don’t shortcut preparation. Hearing the stories and working side-by-side changes the dynamic of the patient-clinical team relationship. This process requires sensitivity and nurturing.
- Pause and consider the likely intensity of the experience you are studying when using ethnographic methods like experience-based design. Plan data collection accordingly. Ensure team members who will gather information are adequately trained and prepared for the task. Think through how you will approach those who had the care experience and how you will handle service recovery if needed.
We  definitely are still developing our skills in this work. But we believe we’re close to reaching the tipping point, where not having our customers’ voices directly involved in improvement feels unthinkable. It is transforming our organization, and that gives us energy to remain vigilant so we can realize that strategic plan goal of putting the patient first.
definitely are still developing our skills in this work. But we believe we’re close to reaching the tipping point, where not having our customers’ voices directly involved in improvement feels unthinkable. It is transforming our organization, and that gives us energy to remain vigilant so we can realize that strategic plan goal of putting the patient first.
Editor’s Note: For the second consecutive year, Virginia Mason was a John Q. Sherman Award Finalist. You can learn more about the scope and impact of their work in their 2016 award nomination.



