



Virginia Mason is an urban integrated health system in the Puget Sound, Washington region, with our flagship campus located in downtown Seattle. Like most healthcare organizations, we strive to actively engage patients in their clinical care. As part of our patient engagement efforts, our patients and their families are directly involved in helping improve our services and processes.
Putting Patients at the Top
Over the past few years, we have accelerated our efforts to involve patients and families directly in improvement activities, guided by our strategic plan that puts the patient at the top to influence all that we do and by our lean management method, the Virginia Mason Production System. A key tenet of our lean-inspired management system is that the customer defines value.
Setting Assumptions Aside
With our long-term commitment to these foundational elements, we have come to understand more deeply how many assumptions we make every day about what matters to our patients and what is shaping their care experiences. For many years, we involved patients and family in organizational activities on a limited scale. We believed that we were listening effectively to the voice of our patients when a patient participated in an improvement workshop or when we channeled patient and family input into our improvement projects to help us define scope and targets. Often, however, there was reluctance to expose our customers directly to our messy processes. In these cases, involvement was at arm’s length, by gathering some satisfaction data and/or customer reactions to ideas being implemented. We needed to rethink how we could truly engage deeply with our customers as we seek to improve their experience of care.
Gathering Experience Stories and Emotional Impacts
As we began learning ethnographic data collection methods and asking our patients and their family members about the emotional impacts of their experiences, the effect was immediate and profound. We began learning to see and listen in a more meaningful, unfiltered way. Combining the emotional experiences and stories from our customers with our other analytical improvement data (lead times, wait times, cycle times, movement, defects, etc.) is bringing the heart together with the head. Both impact the experience and outcomes of clinical care. Patient and family experiences can be a bit of roller coaster, with positive, neutral and negative moments. We gather data about patient/family emotional experiences along with quotes and stories, map these “roller coasters” and use the data to inform our redesign work (We also use this approach with staff as customers of internal processes.).
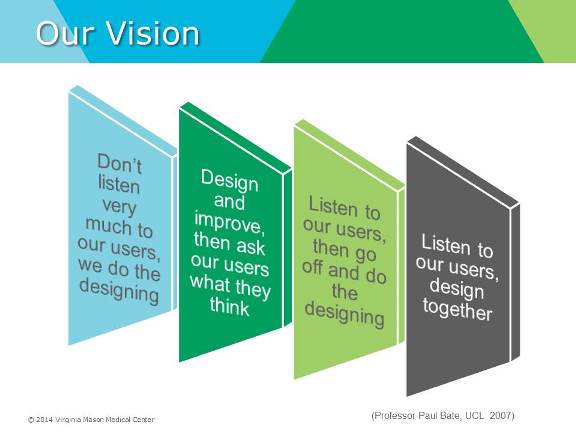
Co-Designing Improvements
In parallel, we’re pursuing a vision to move from designing processes and services for our patients and families to co-designing with our customers. We’re also gathering the voices and involvement of many versus a few. Patients and families are joining projects in larger numbers as equal team members.
A group of patients and family members helped us design the processes needed to get this level of involvement under way. “Don’t treat us with kid gloves,” one family member said. “We want to be put to work, not be a token customer in the room,” another added. They feel insulted and disappointed if they’re invited to participate but it doesn’t feel sincere, or staff are uncomfortable with their involvement. They often are motivated to participate because they want to make things better for other patients. We shouldn’t rob them of that opportunity to contribute.
Things We’re Learning
We must be vigilant to check our biases and avoid defensiveness when we receive customer feedback and input. We use the philosophy of “big eyes, big ears, small mouth” to make sure we’re letting our patients and families tell us their stories, and not react with our long explanations about why “it is what it is.”  In terms of patient-family involvement, you can’t shortcut preparation steps. Do not underestimate the guidance needed to ensure a constructive, rewarding experience. Over time, as our culture continues to transform, the way we prepare individuals and teams may evolve accordingly. Working side-by-side changes the dynamic of the patient-clinical team relationship. Some clinical staff readily take to this, while some are more reticent because it feels counter to their training to preserve some emotional distance. Some patients and family members need minimal orientation and coaching, others need more.
In terms of patient-family involvement, you can’t shortcut preparation steps. Do not underestimate the guidance needed to ensure a constructive, rewarding experience. Over time, as our culture continues to transform, the way we prepare individuals and teams may evolve accordingly. Working side-by-side changes the dynamic of the patient-clinical team relationship. Some clinical staff readily take to this, while some are more reticent because it feels counter to their training to preserve some emotional distance. Some patients and family members need minimal orientation and coaching, others need more.
We must focus on checking our acronyms at the door — slipping into healthcare jargon can feel isolating to our customers. Transparency also is essential. External participants in our improvement projects sign confidentiality agreements and are expected to adhere to privacy policies the same as staff. That means we have to trust them with the same information being provided to the rest of a team.
A Path to Remarkable Care Experiences
Every day, we’re building our skills in these methods and working to make it easier. Our culture is still transforming. But we’re very confident from the work so far that we’re better together, with our patients and families sharing their stories first hand, and rolling up their sleeves to guide us on the pathway to making their experiences more and more remarkable.
Editor’s note: Integrating patients and families into the improvement process has brought about meaningful change at Virginia Mason. It’s no wonder they were a finalist for the 2015 John Q. Sherman Award for Excellence in Patient Engagement.You can read further details about their process and achievements in their award nomination.



