




In December, I discussed the Ever Growing Challenge posed by Frequent ED Users, their prevalence and their characteristics. Here, I’d like to explain why the combination of emergency department (ED) case management, care networks and workflow automation is a pragmatic approach that increases each of the components that encompass value in healthcare – safety, satisfaction and savings.
Big Problem, Bigger Opportunity
The National Institute for Health Care Management reports that 5% of the population is responsible for nearly 50% of healthcare spending. Kaiser shared that 1% of covered lives are frequent ED users who consume 16% of ED resources. Consequently, effective ED visit control represents a substantial opportunity for hospitals to reduce healthcare spending while improving the health status of this cohort.
After HealthPartners began engaging 27 “super utilizers,” their associated ED visits and admissions dropped by 56% and 84% respectively for an annual cost savings of $19,000 per patient. Murphy and Neven further refined the business model for ED case managers focusing on care plan development and compliance. This tactic resulted in reducing visits by two-thirds and cutting over $900 in cost per frequent utilizer (5% of patients) and $4,000 per super utilizer (1% of patients). Following the Annual Volume*$85 formula, potential savings mathematically equate to more than $2 million in an average-volume ED and $11 billion for the U.S. as a whole (since there are 130 million ED visits a year). Additionally, readmissions are prevented, ACO contracts can be leveraged, crowding is relieved and staff is more professionally satisfied.
Engagement Gaps Defined by Category
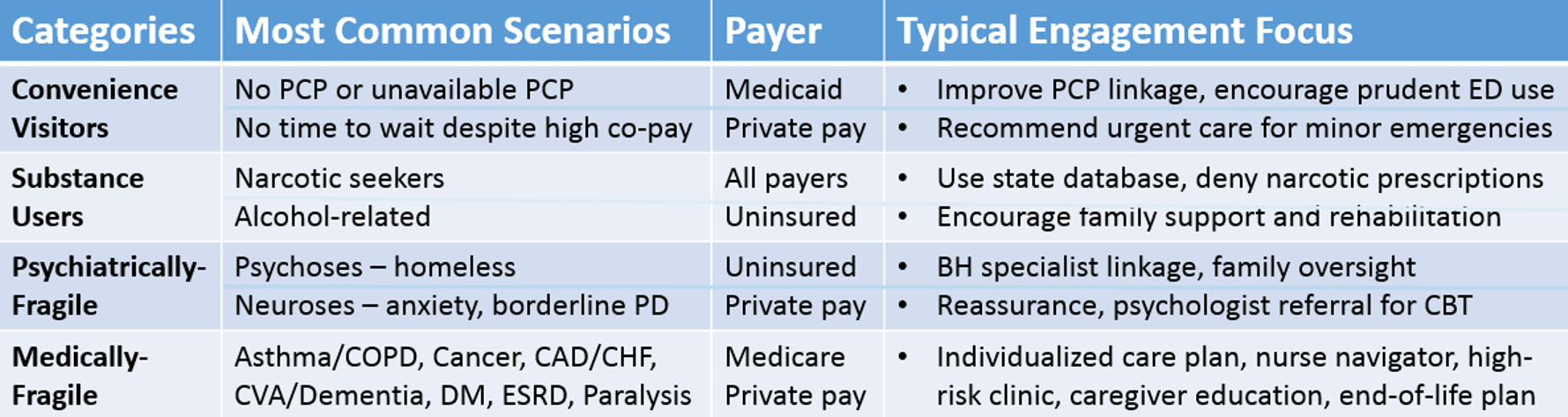
After categorizing frequent ED users consider the vastly different requirements for each group. (See Table).
- Convenience Visitors For this group, the key foci are educating individuals about how and when to utilize more appropriate care resources (e.g., urgent care centers for minor emergencies) and creating linkages to receptive primary care physicians. As well, explaining that we are all accountable for protecting community assets may drive some behavior modification.
- Substance Users The largest group of frequent utilizers are those seeking prescription narcotics to sustain an opiate dependence or to divert these drugs for personal gain. Nowadays, providers can access prescription management databases to confirm (or dispel) any suspicions. Care plans should reflect that narcotics be prescribed only with great discretion. For further recommendations, see Engaging Frequent ED Visitors Seeking Prescription Narcotics.
- Changing the behavior of alcoholics is even more challenging. Family and friends must extinguish all enabling behavior and encourage rehabilitation. Those with cirrhosis, hepatitis, GI bleeding, or pancreatitis must be counselled that such comorbidities are associated with a significantly shortened life-expectancy when alcohol consumption persists. The NHS demonstrated that engaging ED patients with alcohol-related visits is meaningful since for every two brief psychosocial interventions there is one less ED visit over the ensuing 12 months.
- Psychiatrically-Fragile Patients presenting with acute psychosis are usually admitted to a psychiatric hospital. When case managers engage behavioral health specialists, social service options and recruit family members to oversee medication compliance, admission frequency decreases. Patients with anxiety and borderline personality disorders are usually discharged home. They benefit from the ED staff being tolerant and reassuring as well as making psychologist referrals for cognitive behavioral therapy to teach symptom awareness, de-escalation, and impulse control.
- Medically-Fragile It is no surprise that medically-fragile patients require emergency services more than others. Individualized care plans, specialty nurse navigation and high-risk clinic referrals will reduce ED visits and prevent hospitalizations, particularly 30-day readmissions. Primary Care and Emergency Physicians can consider the “illness trajectory” to determine when it becomes appropriate to initiate end-of-life options such as home hospice. As well, educating family caregivers about management of pain, dyspnea, and fatigue helps with crisis management and coping.
Engagement of the Frequent ED User
A Seven-Step Solution
You can see reducing Frequent Utilizers is a complex challenge. Yet, by employing this pragmatic approach, hospital EDs can make significant progress:
- Identify Frequent Utilizers, analyze visit patterns and strive to cut them in half.
- Hire ED Case Managers to engage frequent users, develop care plans and coordinate available resources all in order to improve compliance.
- Flag Care Plan Cases on the ED tracker so that staff can heed recommendations and case managers can periodically update the care plans, which often evolve.
- Recruit Providers such that all primary care physicians, psychiatrists and specialists will each commit to overseeing the outpatient management of a few unattached ED frequenters.
- Engage Family such that an influential relative (or a good friend) that may be willing to help mentor and assist the patient (assuming the patient grants permission).
- Automate Workflows with software to track frequent utilizers, facilitate engagement, simplify care plan enrollment and update the “care network” about visits.
- Measure Success, continually refine the process, and review monthly activity of frequent utilizers in order to demonstrate program effectiveness.
The Bottom Line
ED case management, care networks and workflow automation are essential in controlling frequent ED visitors and this trilogy quite literally helps hospitals transition from volume to value.
References
- National Institute for Health Care Management. The Concentration of Health Care Spending; NIHCM Foundation Data Brief. July 2012. http://www.nihcm.org/pdf/DataBrief3%20Final.pdf
- Kaiser Family Foundation. Characteristics of Frequent Emergency Department Users. October 2007. http://kaiserfamilyfoundation.files.wordpress.com/2013/01/7696.pdf
- Health Partners. Care plans reduce preventable emergency room visits, admissions. 2012. https://www.healthpartners.com/public/newsroom/newsroom-article-list/03-30-12.html
- Murphy SM, Neven D. Cost-effective: Emergency Department Care Coordination with a Regional Hospital Information System. J of Emerg Med. 2014; 47(2):223–231. http://www.jem-journal.com/article/S0736-4679(13)01399-1/fulltext
- Alcohol care teams: reducing acute hospital admissions and improving quality of care http://arms.evidence.nhs.uk/resources/qipp/29420/attachment




3 Comments
Dr. Scaletta – great article. Please consider adding an 8th step. Schedule an appointment with a PCP upon ED discharge to provide the frequent users a medical home. Check out what Milwaukee has accomplished http://mkehcp.org/care-coordination-2/emergency-department-care-coordination/
Since launching the ED Linking project in 2008 with four hospital EDs, the program has grown to include all 10 EDs and FQHCs in Milwaukee County, resulting in over 700 appointments each month with area safety-net clinics. The committee regularly updates its progress in a quarterly report.
The EDCC committee has established a community-wide ED to Medical Home referral protocol supported by MyHealthDIRECT web-based appointment scheduling.
Absolutely, Jeff! The intent was that item #4 would incorporate PCP referral but I agree that this effort is certainly important enough to be singled out and emphasized. I applaud your efforts in Milwaukee to connect EDs and safety-net clinics via an integrated, web-based appointment system – very cool!
To express how we the users or the customers have felt after choosing such a service is actually worth to be shared so that it helps others, actually make things alive, our experiences are really nice keep up.